
The TAS "Report of Breast Thermography Evaluation" is a comprehensive recording and interpretation of the breast thermography examination logically divided into eight sections. Much of the report is self-explanatory; however, it is essential that the practitioner understand the metaphor relating to quantitative data.


Breast Thermogram Image Acquisition Procedure
SET UP:
A) Confirm that the camera is connected to the computer showing a live image,
 and prepared for recording image snapshots.
and prepared for recording image snapshots.
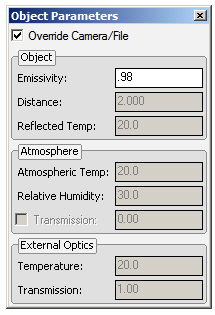
B) Enter "Object Parameters" (emissivity, distance, etc.) and "Recording Settings"
(patient's name, etc.).
IMAGE RECORDING:
A) Position patient for desired view.
Important!
Maintaining camera calibration and focus for different patient views is an easily overlooked discipline. Specifically, the exact distance between the camera and the surface of the patient is a critical parameter for camera calibration, and small changes in camera-patient-distance are often ignored.
Small changes in distance may not be ignored. If the camera-patient-distance changes for each view, and the 'new' distance is not entered as an 'Object Parameter,' the camera is not calibrated, the ability to properly analyze the images is compromised. In short, the examination is tainted.
This issue frequently arises when the patient pivots to accommodate the oblique and lateral views. In the diagram, the patient is initially positioned for a frontal view image, with toes aligned to a line marking the stored camera-patient distance. As the patient pivots for the oblique and lateral views, the camera-patient distance is lengthened.

Camera-patient-distance uncertainty can be minimized by employing specific foot positions for each view. As before, alignment is made to a line marking the stored camera-patient distance:

Important: The end position of the heels for the oblique views is with the heel of the rotated foot against the inside heel of the stationary foot. The patient's weight is supported on the stationary foot. The patient is standing relaxed in natural posture.
Note that for each position, the patient's foot/feet are aligned with the camera-patient-distance line.
B) Assure that the breasts are in focus.
Important: Auto-Focus Is Inadequate!
Impaired viewing and unreliable temperature measurements result when the areas of interest in the image are not in focus. This is a common issue owing to reliance on the camera's automatic focusing mechanism. Unfortunately, the auto-focus feature of infrared cameras is unsuitable for breast thermography examinations.
The camera should be focused slightly in front of the surface of the breast that is perpendicular to the camera. The camera's 'depth of field' maintains image focus for several inches behind the focal point, i.e., the entire breast is in focus.
Auto-focus concentrates on the hottest part of the image. Breasts are cooler than the torso and the axilla and located inches in front of these regions. Using auto-focus, the camera focuses on the torso during frontal views and on the axilla during oblique and lateral views. The breasts are not in focus.
The focus issue is resolved by not using auto-focus, except to initially coarse focus the patient, and then manually touch up focus on the front surface of the breasts.
When the procedure outlined for positioning the patient is adhered to, the distance between the camera and the front of the surface of the breast remains constant. There is no need to refocus for each patient position.
C) Capture the image, and confirm image integrity and quality.
D) Repeat Steps A), B) and C) for each view.
E) After all images have been recorded checked for and their integrity established,
 the examination is ready to be submitted to TAS for evaluation and reporting.
the examination is ready to be submitted to TAS for evaluation and reporting.
Press 'Continue' on the form for the Submit Page.
SUBMITTING EXAMINATION & IMAGES FOR INTERPRETATION
Submitting the recorded images and examination information required to evaluate the patient for risk is a straight forward procedure. First, the form, below, is completed for the examination.

After the above form has been completed, click 'Submit Information and Continue.' This will launch the 'Image Uploading' page:

Selecting the images is accomplished by clicking on 'Add files.' This launches the standard Windows file selection dialog. It should already be 'pointing' to the folder where new images are stored, if not, navigate the dialog to the folder. Select ALL files that you desire to submit by holding down the Ctrl key and clicking the left mouse button on each file you want to include with the examination. Then, click 'Upload Selected Image Files.' After a few moments, you will receive screen confirmation of the successful upload.
Should you receive an error message instead of an acknowledgement of successful upload, it will be necessary to repeat the examination submittal process.
Reviewing the Findings Report
Click image for full-size report
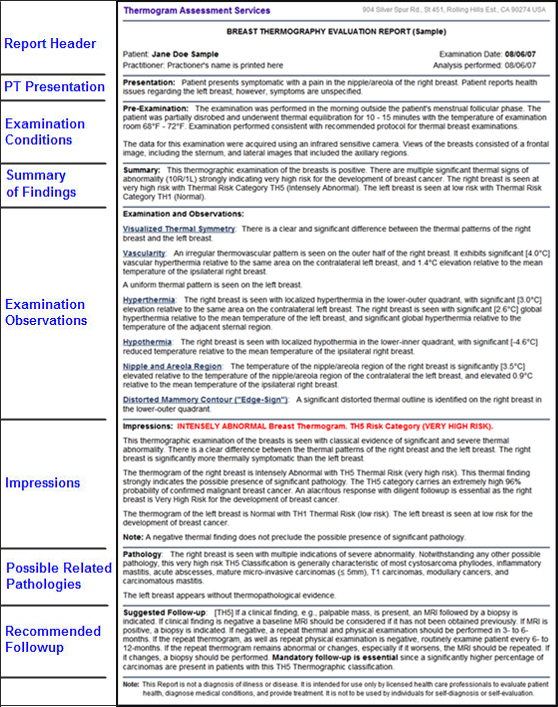
I. REPORT HEADER
Thermogram Assessment Services
18484 Preston Rd., Ste 102-142, Dallas, TX 75252 USA
REPORT OF BREAST THERMOGRAPHY EVALUATION
Patient: Jane Doe
Examination Date: 08/06/07
Practitioner: Practitioner's name is printed here
Analysis performed: 05/28/07
Practice: Referring practice name is printed here
II. PATIENT PRESENTATION
Presentation:
Patient presents symptomatic with a pain in the upper half of the right breast. Patient reports health issues regarding the left breast; however, symptoms are unspecified.
The Patient Presentation Section records the patient's stated purpose for undergoing the thermographic examination. The Section excludes any clinical findings.
III. PRE-EXAMINATION CONDITIONS
Pre-Examination:
The examination was performed in the morning outside the patient's menstrual window of activity. The patient was partially disrobed and underwent thermal equilibration for 10 - 15 minutes with the temperature of the examination room 68°F - 72°F. Examination performed consistent with recommended protocol for thermal breast examinations.
The data for this examination were acquired using an infra-red-sensitive camera. Views of the breasts consisted of a frontal image, including the sternum, and lateral images that included the axillary regions.
The data for this examination were acquired using an infra-red-sensitive camera. Views of the breasts consisted of a frontal image, including the sternum, and lateral images that included the axillary regions.
Knowledge of pre-examination conditions is an important aid to understanding images of the instant examination, and it's an important data reference for future and serial thermographic examinations, which should be performed under the same [acceptable] conditions.
The data presented in the Pre-examination Conditions Section reflect the practitioner's preferences selected in the Register New Account process, modified if necessary, when completing the Examination Information Form.
IV. SUMMARY
Summary: This thermographic examination of the breasts is seen with classical evidence of severe thermal abnormality.
There is a clear difference between the thermal patterns of the right breast and the left breast.
The right breast is significantly more thermally symptomatic than the left breast.
The Right breast is Intensely Abnormal (Very High Risk) with Thermal Risk Factor TH5. The Left breast is Normal (Low Risk) with Thermal Risk Factor TH1.
The Summary abbreviates examination findings, but employs adjectives to key words for increasing statement weight consistent with increased severity of examination results.
When neither breast presents as exceeding Normal (THI) Classification, the statement is generated, 'This thermographic examination of the breasts is seen without evidence of thermal abnormality.' If, however, either breast exceeds Classification THI, but neither exceeds Borderline Normal (THII) Classification, the keyword 'without' is replaced by the keyword 'with', e.g., 'This thermographic examination of the breasts is seen with evidence of thermal abnormality.'. This statement is further modified depending on the severity of examination findings.
If either breast presents as, but neither breast exceeds Borderline Abnormal (THIII) Classification, the keyword evidence is amplified to classical evidence. Similarly, if either breast presents as Abnormal (THIV) or Severely Abnormal (THV), the phrase thermal abnormality is qualifed with the adjective 'severe' to read severe thermal abnormality. Consequently, the statement, 'This thermographic examination of the breasts is seen with classical evidence of severe thermal abnormality' serves to inform the practitioner that the patient's examination result indicates serious abnormality.
The statement 'There is a clear difference between the thermal patterns of the right breast and the left breast' arises when either the analyst mandates it by analyst response, or when the program detects significant differences in the thermal signatures of the two breasts.
The message 'The right/left breast is more thermally symptomatic than the left/right breast' appears when one breast's thermal score exceeds the thermal score of the other breast. If the difference in thermal score exceeds a preset threshold, the modifier 'significantly' precedes 'more thermally symptomatic,' e.g., 'The right/left breast is significantly more thermally symptomatic than the left/right breast
V. EXAMINATION AND OBSERVATIONS
Examination and Observations:
Vascularity:
A thermovascular network is seen on the upper half of the right breast.
It exhibits slight (1°C) vascular hyperthermia relative to the same area on the contralateral left breast, and slight (1°C) intensity relative to the mean temperature of the ipsalateral right breast.
A uniform thermal pattern is seen on the left breast.
Hyperthermia:
A minimal (1°C) local/regional hyperthermia is noted on the upper-outer quadrant of the right breast.
There is mild total hyperthermia of the right breast relative to the mean temperature of the left breast and relative to the temperature of the adjacent sternal region.
Hypothermia:
A severe (-4°C) localized hypothermia with significantly reduced temperature relative to the mean temperature of the right breast is identified on the lower-outer quadrant of the right breast.
Nipple/Areola Region:
The temperature of the nipple/areola region of the right breast is mildly elevated (1°C) relative to the contralateral left breast nipple/areola.
The nipple/areola region of the right breast is slightly elevated (1°C) relative to the mean temperature of the ipsilateral right breast.
The nipple/areola region of the left breast is slightly elevated (1°C) relative to the mean temperature of the ipsilateral left breast.
Distorted Mammory Contour ("Edge-Sign"):
A distorted thermal outline is identified on the lower-outer quadrant the right breast.
The Examination and Observations section of the Breast Thermography Report offers amplified insight to the condition of the patient's breast health. It serves to document the analyst's observations, which is especially useful in the context of serial thermograms. In furtherance of assisting this important procedure, the Gautherie interpretation protocol upon which this program is based is augmented to record a thermographic history of the patient's examinations.
By way of review, Gautherie assigns a thermal score to situations where a variable exceeds a specific threshold. For example, a local hyperthermia exceeding 2.5°C contributes 30 'points' to the total thermal score of the breast exhibiting the hyperthermia. If a hypertheria is less than 2.5°C, no points are contributed.
TAS has augmented the Gautherie technique by remarking on observations that would not be otherwise noted using Gautherie's scoring thresholds, and by computing an "Augmented Thermal Score" based on fractional scoring that is dependent on the observation. In the example case, a 2.0°C hyperthermia, approximately 63% of Gautherie's threshold, would contribute about 20 points to an Augmented Thermal Score.
If no abnormality is observed or noted by the program, no statement is given. Five categories delineate the level of importance of observed thermal signs. They, or with similar labels, and their respective statistical break points, are characterized with different keyword modifiers. They also include recording of pertinent temperature for future reference. The five categories of observed thermal signs are:
- Slight: The word 'slight' refers to a thermal marker that is greater than zero, but less than the lowest temperature difference contributing points to the total thermal score. This is generally 50% of Gautherie's scoring threshold.
- Mild: A 'mild' category observed temperature difference falls between 50% and 63% of Gautherie's scoring threshold temperature difference. It contributes 50% of Gautherie's score to the Augmented Thermal Score. This sign should not be overlooked, as it, along with other signs, may indicate a breast disorder.
- Moderate: 'Moderate' category remarks indicate the observed thermal sign exceeds 63% and is below 82% of Gautherie's scoring threshold temperature difference. It contributes 63% of Gautherie's score to the Augmented Thermal Score. This sign should not be overlooked, as it, along with other signs, may indicate a moderately serious breast disorder.
- Borderline Severe: Observations characterized 'Borderline Severe' exceed 82% of Gautherie's scoring threshold temperature difference. These are close to contributing to Gautherie's total scoring, and contribute 82% of Gautherie's score to the Augmented Thermal Score. This sign, along with other signs, may indicate a moderately serious breast disorder.
- Severe: Observation remarks in the 'Severe' category equal or exceed the Gautherie protocol threshold and thus contribute 'points' to the Total Thermal Score using Gautherie's protocol, as well as the Augmented Thermal Score. Again, this sign, along with other signs, may indicate a moderately serious breast disorder.
Note: Observations in the Severe Category are characterized with the word 'severe' and scored 100% in conformity with the Gautherie interpretation protocol.
VI. IMPRESSIONS
Impressions: INTENSELY ABNORMAL BREAST THERMOGRAM. TH5 [VERY HIGH RISK] CLASSIFICATION.
The right breast is seen at very high risk for the development of breast cancer, presenting a Thermal Classification TH5.
This is Intensely Abnormal (Very High Risk). This thermal finding statistically indicates the presence of significant pathology. Immediate attention is recommended.
The left breast is seen at low risk for the development of breast cancer, presenting a Thermal Classification TH1.
This is a Normal (Low Risk) breast thermogram.
Note: A negative thermal finding does not preclude the possible presence of significant pathology.
VII. PATHOLOGY
Pathology:
The right breast is seen with multiple indications of severe abnormality. Notwithstanding any other possible pathology, this very high risk TH5 Classification is generally characteristic of most cystosarcoma phyllodes, inflammatory mastitis, acute abscesses, mature micro-invasive carcinomas (≤ 5mm), T1 carcinomas, modullary cancers, and carcinomatous mastitis.
The left breast appears without thermopathological evidence.
Impressions and Pathology are seperate, but closely related sections of the Breast Thermography Report. The Impressions section speaks to the program's assessment of the patient's breast health condition and risk of developing breast cancer. The Pathology Section speaks to the pathologies typically seen for such impressions.
VIII. RECOMMENDED FOLLOW-UP
Recommended Follow-up:
[TH5] If a clinical finding, e.g., palpable mass, is present, an MRI followed by a biopsy is indicated. If clinical finding is negative a baseline MRI should be considered if it has not been obtained previously. If MRI is positive, a biopsy is indicated. If negative, a repeat thermal and physical examination should be performed in 3- to 6-months. If the repeat thermogram as well as repeat physical examination is negative, routinely examine patient every 6- to 12-months. If the repeat thermogram remains abnormal or changes, especially if it worsens, the MRI should be repeated. If it changes, a biopsy should be performed. Mandatory follow-up is essential since a significantly higher percentage of carcinomas are present in patients with this TH5 Thermographic classification.
The Recommended Follow-up section serves only as a guideline to what appropriate procedures to follow depending upon thermographic impressions. Note that other acceptable diagnostic modalities should never be ruled out for symptomatic patients, even when thermographic results are negative. A negative thermal finding does not preclude the possible presence of significant pathology.